Announcing (yet another!) attempt to get the global perspectives on Oncology on a singular platform. I’ll address this through FAQ’s.
Q. Why is this needed?
A. This attempt has been borne out of frustration with social media- Twitter/Facebook/Instagram etc. where users get together. Algorithms determine everything. Your timeline, visibility and your “tweetorials”. Your ranking (and being heard by others) is now determined by your financial capacity. It shouldn’t have been the case. #medtwitter has outlived it’s life.
Q. Why is it fundamentally wrong?
A. Quitting social media is considered as “career suicide”. Therefore, despite the burn-out, we persist. The acceptance of our ideas is loosely measured by retweets and likes on our posts. Real-life scenarios require persuasion, instead. We need to sound convincing to our peers/patients. Claims of thousands of retweets on your tweets have no bearing on your opinion in tumour board or when we are trying to convince our patients for stereotactic ablation.
Q. How should I balance professional/personal commitments and pursue academic goals as well?
A. This is a tough call. Our motivation gradually dwindles as we age. Commitment towards our family goals requires a fine balancing act and aligned with our duties and responsibilities towards our patients. There are several ways to achieve reading/writing goals by time-management and identification of “time-sinks” (activities that take away our attention- like doom-scrolling on Twitter/Instagram).
Q. But, there are tweetorials (and conferences)
A. As yourself these questions (and be honest to self):
- How many tweetorials can you consume in a day?
- Do you get the context of the argument?
- Is it practise changing or you are only there for the survival curves/”key-takeaways”?
- Can you reliably poke holes in the published arguments?
- Does it positively impact your patient-care?
- When was the last time you can reliably recall what you “heard/read” in a conference? Is knowing the immunotherapy combination (as an example) relevant to your current practises? Were there any alternatives considered? Do financial disclosures even matter?
Q. Quasi-movements towards “inclusivity” and more “good-sounding” jargon
A. New movements (and as “counter-culture) like the “hippies” come and go. I have seen them exhorting users through editorials/banners and “committed individuals”. Yet, they miss the point. They fear “agenda-dilution”. They fear embracing disruption. They fear losing control. What’s the point?
Q. Community practises versus academia
A. This is a “sore-point”. Few individuals have managed seamless transition, and there are many spins to the tale. A general impression is around “original-thinking” happening in academia- witness the breathless announcements on #medtwitter around “innovative-breakthroughs” and “late-breaking abstracts”. Yet, it’s the “community-practise” (behind the trenches) where work gets done with ALL the inherent limitations. Academia has an entire team to grind towards “publications” but patient-care happens across the spectrum. Many ideas don’t get funded because of prevalent bureaucratic hurdles/grant systems. Many countries don’t even have that equivalent system. Yet, patients get treated. Both across academic centres AND the “community-hospitals/private facilities”.
Q. Why we still then need to “congregate”?
A. Congregate. Origin: Latin “congregatus”, past participle of congregare “to herd together, collect in a flock, swarm; assemble,”. It is the inherent need; an impulse. A “social-need” and a “social-contract”.
Q. How does learning happen, then?
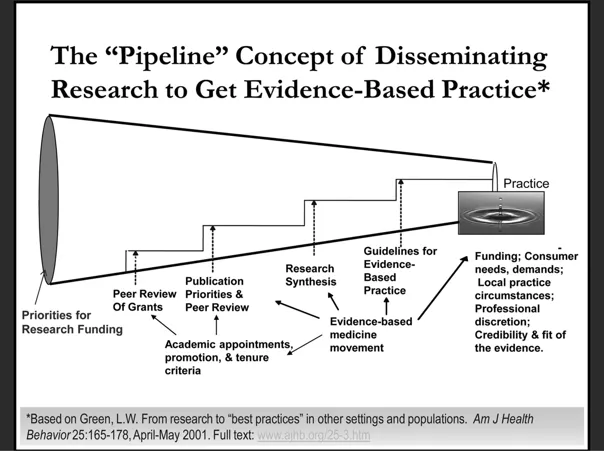
A. Glad you’ve asked! Here’s the “fallacy of learning”:
Quick points to summarise:
- There is often a disconnect between learning/research and putting that knowledge into practice, especially in public services.
- The hierarchical model of training and knowledge transfer, where experts deliver information to passive recipients, is ineffective for complex real-world implementation.
- Factors like confirmation bias, projection bias, and contextual constraints mean people don’t simply absorb and apply new information, but filter it through their existing beliefs and experiences.
- Sharing failures and negative results is important, as it helps avoid repeating mistakes, but organizations often discourage this due to a culture of blame.
- There needs to be a “pull” approach that brings research closer to the actual circumstances of practice, rather than a “push” of academic knowledge onto practitioners.
- Participatory research strategies that involve practitioners and communities are more likely to produce actionable, relevant evidence.
- Hierarchical structures in organizations and between organizations/communities create barriers to knowledge sharing and implementation.
- Networked, collaborative models where power is distributed can be more effective for complex problem-solving.
- Timeliness is crucial – the 17-year lag between research and patient benefit is unacceptable in the digital age.
- Embracing the complexity of real-world environments, rather than trying to control for it, is key to effective knowledge application.
Q. What is the most logical way forward?
A. Thank you for reading till here. I have implemented a telegram group to take this forward:
- No algorithms. Zero.
- No hierarchies. That’s the aim. We are all students till we come to the ungodly realisation that we know the “topic”.
- Symmetric flow of information with gradual exchange of information between participants from across the world.
- Imagine and mull over this: cancer cells have beautiful intricate intercellular signalling/communication systems. We, those who “cure”, have biases, prejudices, perceived hierarchies, “hesitation”, preconceptions. Who’s smarter?
- Gamification. Rely not on the algorithms but peer filter to gain “points”. You remain visible at all times. Your financial capacity doesn’t enter into equation here.
- Foster a global thinking and create a conducive learning.
- I have nothing else but trust and technical know-how to offer.
Q. I am excited/enthusiastic/eager/curious to know more and wish to join. How can I do that?
A. Simple:
- Download Telegram
- Register for the service.
- Create a username (not mandatory, but it helps). You don’t have to share your phone number to interact with anyone on Telegram. Username is suffice.
- Explore privacy features on Telegram. (spoiler alert: They are AWESOME).
Link for Telegram Group:
You can join here: https://t.me/+1cPyUl3WW8IxOTk1
